A 55-year-old man with a history of COPD presents to the emergency room with two days of worsening shortness of breath following a recent viral infection. In the emergency room, his oxygen saturation in room air was 88%. He struggled to breathe and spoke only very short sentences. On examination, he had diffuse wheezing and a prolonged expiratory phase. His chest x-ray showed changes consistent with COPD but no new focal infiltrates. An arterial blood gas analysis (ABG) was performed and showed pH 7.17, PCO2 55, PO2 62, and HCO3-25.
What are the indications for initiating mechanical ventilation in the patient?
There are several major indications for initiating mechanical ventilation, including: hypercapnic respiratory failure, hypoxic respiratory failure, preventing or reversing pulmonary atelectasis, preventing or reversing ventilatory muscle fatigue, allowing sedation and/or neuromuscular blockade (e.g., surgery), stabilizing the chest wall (e.g., a large continuous chest), or ensuring airway protection (e.g., patients with altered mental status and massive upper gastrointestinal bleeding).
One should be aware that for hypercapnic and hypoxemic respiratory failure, there is no specific threshold for determining when to initiate mechanical ventilation. For example, you will not automatically intubate a patient when PCO2 rises above 60 mm Hg or when room air PO2 drops below 55 mm Hg. Instead, you must consider the entire clinical picture and assess whether the degree of hypercapnia or hypoxemia is life-threatening to the patient. You may delay initiating mechanical ventilation if they can be supported by other means, such as mask oxygenation, whereas if their PO2 continues to fall despite higher levels of supplemental oxygen, mechanical ventilation is required. Similarly, you may try mask oxygenation for hypoxic respiratory failure if the patient is hemodynamically stable, but if the patient exhibits signs of sepsis, hemodynamic instability, and multiorgan dysfunction, you can intubate the patient more quickly and stabilize their respiratory status so that you can focus on other important issues.
How do you see the possibility of using non-invasive positive pressure ventilation (bi-level positive airway pressure ventilation) in this patient?
There are two forms of mechanical ventilation – invasive mechanical ventilation, in which an endotracheal tube is inserted into the patient’s airway, and noninvasive ventilation, in which the patient receives respiratory support through a tight-fitting mask worn over the face. In some cases, invasive modes of mechanical ventilation are necessary, while in other cases, patients can be supported by noninvasive means.
This patient falls into the latter category. Despite his obvious respiratory distress, elevated PCO2, and decreased pH, it was reasonable to give him a trial of noninvasive ventilation. There is now a wealth of data suggesting that patients with COPD exacerbations and hypercapnia can be successfully treated with noninvasive ventilation; this strategy reduces the need for intubation and initiation of mechanical ventilation, improves survival, and shortens ICU length of stay compared with patients who are not ventilated noninvasively (e.g., using only mask oxygenation). Given the data in this regard, this patient should undergo a trial of noninvasive ventilation and be closely followed for his respiratory status. If he improves, he can continue noninvasive ventilation, but if his oxygenation or hypercapnia worsens under optimal noninvasive ventilation conditions, or if he becomes unresponsive or uncooperative, he will require intubation and invasive mechanical ventilation.
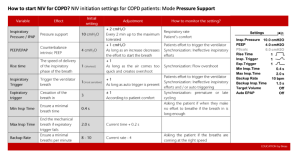
In CPAP therapy, a constant level of pressure is applied to the airway throughout the respiratory cycle (inspiration and expiration). This pressure is used to avoid pulmonary atelectasis and improve oxygenation by opening the large airway and preventing alveolar collapse. There is no additional pressure transfer during inspiration and therefore no ventilatory support. In bi-level positive airway pressure ventilation (also called non-invasive positive pressure ventilation), the expiratory pressure applied to the airway during exhalation is the same as the pressure applied during CPAP therapy. During inspiration, the device applies additional pressure to the airway (pressure support or inspiratory assist) to assist the ventilatory muscles in their efforts to produce an inspiratory airflow to the alveoli.
What is the difference between bi-level positive airway pressure ventilation (BiPAP) and continuous positive airway pressure ventilation (CPAP)? What are the indications for using these different modes of noninvasive mechanical ventilation?
These differences in the way CPAP and bi-level positive airway pressure work have a significant impact on the clinical situations in which they can be used. CPAP is indicated for the treatment of obstructive sleep apnea because of its effect on transmural pressure and its ability to prevent upper airway collapse. There are also data supporting its use in patients with cardiogenic pulmonary edema; the applied pressure improves oxygenation by opening the alveoli. CPAP also improves hemodynamics in cardiogenic pulmonary edema by reducing afterload and preload, thereby improving left ventricular function. Due to the increased pressure during inhalation, bi-level positive airway pressure provides a way to support ventilation and work of breathing. There are clear data supporting its use in COPD exacerbations and in patients suffering from other forms of ventilation failure, such as amyotrophic lateral sclerosis and myotonic dystrophy. Although many clinicians routinely trial this treatment in asthmatic patients during asthma exacerbations, there are no clear data to support its use in asthma exacerbations. There are also some data suggesting that it has a role in the treatment of patients with neoplastic pneumonia. CPAP does not provide any ventilatory assistance and therefore should not be used in these situations.